Ankle Anatomy
The structures of concern for the ankle include 4 major bones, 3 major ligaments with a further grouping of ligaments.
There are 6 major muscles that play a key role in controlling the ankle with the help of a nerve supply.
The bones and ligaments provide the ‘passive stability’ to the ankle. It’s these six muscles that provide the dynamic stability.
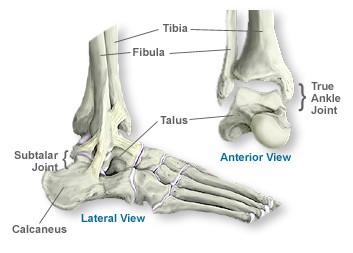
Bony anatomy
- The ankle joint is created by the talus bone and the lower ends of the fibula and tibia.
- The talus sits between these two long bones of the lower leg, with the fibula on the outside and the tibia on the inner-side, creating the bony sides of the ankle
- The bony landmarks are the lateral malleolus (fibula) and the medial malleolus (tibia)
- Situated under the talus is the calcaneum (better known as the heel bone)
- The joint between the talus and the calcaneum is the subtalar joint
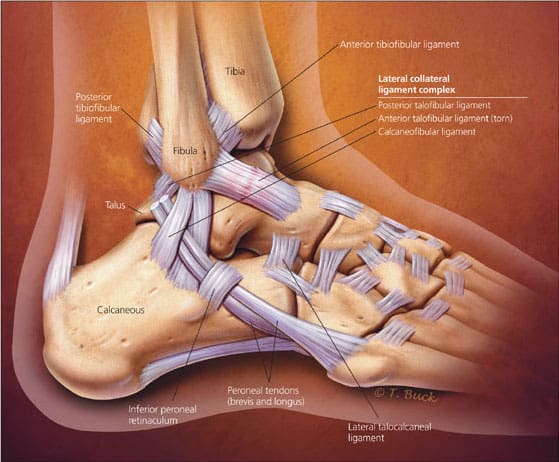
Ligament anatomy
- The ligaments involved on the outside of the ankle are the anterior talo-fibular ligament (ATFL), calcaneo-fibular ligament (CFL) and the posterior talo-fibular ligament (PTFL) on the outside and the deltoid ligament on the inner side of the ankle
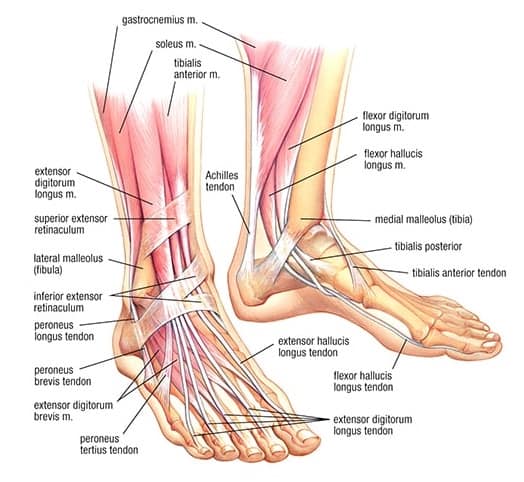
Muscle anatomy
- The 3 most notable muscles of the ankle for dynamic stability are the two peroneal muscles on the outer side (peroneus longus and peroneus brevis) and the tibialis posterior muscle on the inside.
- Three other important muscles are the gastrocnemius and soleus which together make up the calf, and tibialis anterior that runs along the front of the ankle.
- Together, the talocrural and subtalar joints allow the foot to move in all directions
- Ligaments provide ‘passive stability’, ie they limit the joint range of movement
- The muscles provide movement and ‘dynamic stability’ to the joints ie they control movement before reaching end of range.
Nerve anatomy
Let’s not forget these super important anatomical structures – the nerves.
Nerves are critical to coordinating movement, and providing feedback to the brain about ankle position and the effect of muscle activity.
The tibial nerve is located on the inside of the ankle and the sural nerve on the outside of the heel. At the front of the ankle are the superficial and deep peroneal nerves.
The sural nerve is often involved in inversion injuries due to being stretched or tractioned when the ankle rolls over.
What happens in an ankle sprain?
- Inversion ankle sprains are the most common form of ankle sprain, involving the structures of the outside of the ankle
- This can occur when landing awkwardly on the outside of the foot or stepping onto uneven ground, causing all of the weight to go onto the outside of the foot
- When the ankle is forced into inversion, the ATFL and CFL most notably are put on stretch. If this force exceeds the tolerance of the ligament, it will be strained
- The peroneal muscles are usually put on stretch as well, which usually causes more of the bruising for an ankle sprain
- The peroneals are usually active in attempting to control the inversion movement, which can result in an avulsion fracture of the base of the fifth metatarsal
- The sural nerve is also put on stretch, its injury contributing to pain and sometimes producing altered sensation on the outside of the foot