Vertigo and dizziness can be truly debilitating and can severely affect a person’s quality of life. The most common cause of vertigo is Benign Paroxysmal Positional Vertigo (BPPV).
BPPV is a disorder of the inner ear that causes dizziness, vertigo, unsteadiness, and nausea when a person moves their head.
Although the condition can be extremely unpleasant, with the right physio assessment and treatment it can be resolved fast.
In this article, we will delve into the details of BPPV, including relevant anatomy, its causes, symptoms, diagnosis, and treatment.
This article is worth reading if you:
- suffer from dizziness from time to time, or you know someone who does
- have heard the term BPPV and wonder if this is your problem
- have been given anti- nausea tablets for your dizziness but wonder if there is anything else you can do
At the end of this article, you’ll understand:
- how Benign Paroxysmal Positional Vertigo (BPPV) happens
- the anatomy of the vestibular system
- what causes BPPV
- the best treatment for BPPV
REMEMBER: Not All Vertigo Is BPPV!
There are many causes for vertigo and dizziness.
BPPV just happens to be a common cause!
Anatomy to help you understand BPPV
The purpose of our vestibular organ is to detect our head position and head movement.
The vestibular organ is one component of your inner ear. The other component is the cochlea, which is dedicated to hearing.
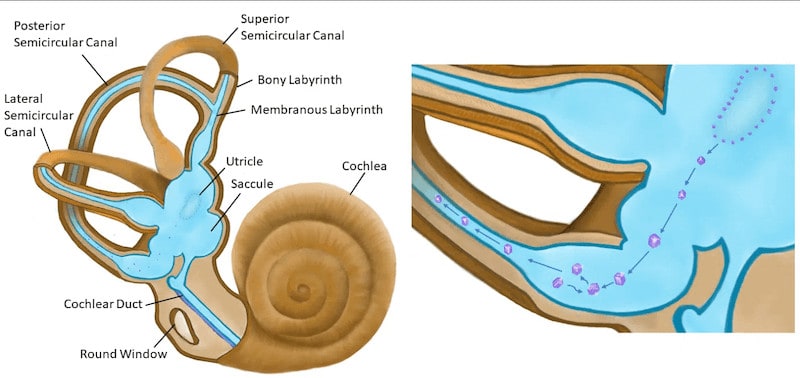
Your vestibular system is made up of two parts – the otolith organs and the three semicircular canals.
Within the otolith organs, there are calcium carbonate crystals (often called otoconia, or just ‘crystals’) that add weight to a membrane.
Movement of the substance under the membrane bends specialised hair cells. It’s these hair cells that detect the position of your head and head movement.
The other part of the inner ear balance system is the fluid-filled semicircular canals. Within each inner ear, there are three semicircular canals: a superior, a lateral and a posterior semicircular canal. These contain fluid, called endolymph, which moves freely within the canals.
If you turn your head at speed, the fluid stays still while your head moves. That is, the canal moves in relation to the fluid.
The direction of head movement determines which semicircular canal is involved. The arrangement of the semicircular canals allows the detection of movement in three dimensions.
The movement of the fluid (or the movement of the head in relation to the fluid) is detected by more specialised hair cells which generate a signal to the brain that you have turned.

What is Benign Paroxsymal Positional Vertigo (BPPV)?
BPPV is a common inner ear disorder and the most common cause of vertigo.
People of all ages can be affected by BPPV, but it is particularly common in people over the age of 65 years old.
BPPV happens when a fragment of the calcium carbonate happens to break free from its normal location in the otolith organ and find its way into one of the semicircular canals.
The fragments plus the altered flow of the endolymph inadvertently create incorrect messaging, so that you feel the illusion of movement, which can feel like spinning or falling.
The most commonly affected canal is the posterior semicircular canal.
The feeling of vertigo is only present while the crystals or fluid are moving, so when it stops, the vertigo feeling settles.
People that suffer from BPPV can usually describe specific activities that set off their vertigo symptoms. Common triggers include rolling over in bed or looking upwards.
What are the symptoms of BPPV?
BPPV creates a sensation of vertigo, which can feel like either you or the room spinning, or that you are falling. The direction of spinning or falling will depend on the affected canal.
The usual pattern is that this spinning or falling sensation eases within a minute.
The intensity of the vertigo can range from mild to severe.
There is often no sensation of vertigo or dizziness apart from after doing the triggering movement, but instead there can be a sense of lingering unsteadiness.
Nausea and vomiting are often a consequence of this sensation. This is because the visual information and other bodily signals don’t match with the vestibular information. The mismatch between the different sources of data is nauseating.

What causes BPPV?
There are a few proposed reasons for BPPV.
One is some kind of head trauma that allows a crystal to break free.
Another possible reason is a consequence of inner ear infection.
It is suggested that age-related changes to the otolith organs could be a reason why it is more prevalent in the over 65 age group.
How is Benign Paroxysmal Positional Vertigo diagnosed?
The diagnosis of BPPV can be made from your symptom behaviour and the results of physical testing. There is no imaging that will diagnose BPPV.
Keeping in mind that BPPV is one of many possible reasons for dizziness, it is important for us to:
- fully understand the behaviour of the dizziness or vertigo
- understand any other features in someone’s condition or general health that would help to differentiate between BPPV and another cause.
One of the key pieces of information is the particular movements or activities that trigger BPPV symptoms, and the duration of the vertigo when that movement is performed.
There is a series of physical tests that are used to help determine
- if it is truly BPPV
- which semicircular canal is involved
- which side is effected
The particular test which provokes dizziness and the direction of eye movement (nystagmus) allows the diagnosis to be made.
Although this sounds horrible, the vertigo that it provokes settles quickly within a minute.

Physio treatment for BPPV
Benign Paroxysmal Positional Vertigo can subside with time, but the duration for natural resolution varies a lot.
During the time that dizziness is present, there is an increased risk of falls and further injury. Therefore, it is wise to seek treatment early and get your BPPV treated.
BPPV can usually be treated successfully with specific movements that are perfomed by your physio.
The key repositioning manouevres are called the Epley manouevre and the Gufoni manouevre.
It is important that the correct exercise is used for the affected ear so that symptoms improve and instead of worsened.
The goal of these manouevres is to guide the otoconia out of the semicircular canals and back into the otolith organs., so that they no longer are providing incorrect and misleading information to the brain about movement.
The good news is that resolution often happens quite quickly. Sometimes the vertigo is completely eradicated in the first session, sometimes followup sessions are required. Repeating the movement at home can also be prescribed.
Motion sickness medications may be prescribed by your general practitioner to make the BPPV episode easier to recover from, but following the clinical practice guidelines mean using vestibular rehabilitation techniques performed by a physio.
For many people, particularly in the older age group, additional balance exercises are useful following BPPV.
It is worth noting that people who have had a history of vestibular neuritis are more likely to be slow responders or have residual feelings of dizziness or imbalance, even if it no longer is true vertigo.
If symptoms persist despite following the vestibular rehabilitation program, it is worth consulting your general practitioner for further investigation to see if there is another cause for your vertigo.
Other causes for Vertigo or dizziness
It is worth stressing that there are many causes for dizziness and vertigo, and that BPPV is just one of them.
Other possible causes are:
- Meniere’s disease
- viral infection causing vestibular neuritis
- vestibular migraine
- blood pressure
- medication side effects
Another common cause of dizziness is the upper cervical spine which can be (but not always) accompanied by headaches or neck pain.
It also worth highlighting that stress and anxiety can cause dizziness sensations.
So how do you work out what is causing your dizziness?
Ring us to make an appointment with one of our physios, and mention that you have a dizziness problem.
We can direct you to the physio who will suit you the best!
Summary
- The most common cause of vertigo is benign paroxysmal positional vertigo (BPPV).
- BPPV is a common disorder of the balance system of the inner ear that causes dizziness, vertigo, unsteadiness, and nausea when a person moves their head in certain ways.
- Benign paroxysmal positional vertigo is caused by small crystals in the inner ear becoming dislodged and moving into one of the three semi-circular canals, affecting the flow of fluid and giving the illusion of movement or spinning.
- Symptoms of BPPV include vertigo triggered by certain movements, unsteadiness, and nausea or vomiting.
- Benign paroxysmal positional vertigo can be caused by head trauma, inner ear infections, or age-related changes to the otolith organs.
- Diagnosis of BPPV involves questioning about the behaviour of the dizziness or vertigo, as well as physical testing.
- Treatment for benign paroxysmal positional vertigo typically involves simple exercises such as the Epley’s maneuver or Gufoni maneuver