
ACL injury prevention programs
Prevention is key – it’s the best way to avoid ACL injury and surgery.
Prehab is exercise that is done before injury to reduce the risk of injury. It is preventative exercise.
The FIFA 11+ program and the Netball Australia KNEE program are two ACL prevention programs that have been developed within the last 10-15 years.
They are research-based programs that have been designed to help lower ACL injury rates in their chosen sports.
Both programs incorporate a mix of running, strength, plyometrics and single leg control.
Both programs also have the flexibility to progress the exercises depending on an individual’s requirements and capabilities.
They are also designed to both be completed within roughly 20 minutes.
Interestingly, not only are both programs incredibly effective at reducing the rate of ACL injuries, but lower limb injuries in general.
Check out the reductions in injuries from the FIFA 11+ program below. It is pretty impressive.
Results of the FIFA 11+ programme
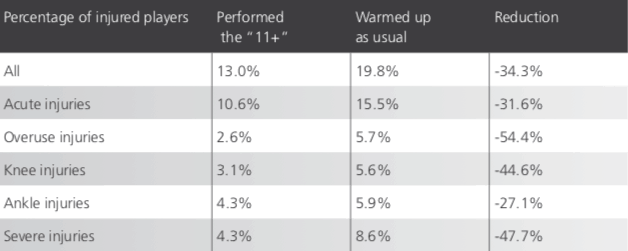
Those results are amazing.
Reducing knee injuries by nearly 50%, reducing overuse injuries by more than 50% and reducing overall injuries by a third is very impressive.
Better still, all of the incorporated exercises were designed to be performed anytime, anywhere.
All they require is the ball of choice and enough space to perform the running sections of the drills.
The role of physiotherapy in ACL injury
Physio treatment helps:
- reduce initial pain and inflammation,
- returning your joint its normal full range of motion,
- strengthening and lengthening supporting muscles where needed
- improve balance & proprioception,
- improve agility
- return to normal functional tasks such as running, squatting, jumping and landing
- minimising the chance of re-injury.
Principles of ACL rehabilitation
5. The final stage is gradually increasing sport-specific drills and training loads until the player has returned successfully to full training, followed by a return to game play.
Confidence is something that takes a while to recover and often comes in waves throughout the rehabilitation process. In order to return to training and competition, it is important not to feel any sense of hesitancy with the knee. This is a critical factor in returning to sport.
Final thoughts
If you are currently involved with sports or have kids who are, I highly recommend looking into these programs as a good starting point to ensure you are being proactive about preventing injuries.
Incorporating these programs is one step to improving you performance and keeping yourself on the field.
The links to both of the booklets are below:
FIFA 11+ https://www.sportsphysiotherapy.org.nz/documents/Injury%20prevention/fifa%2011.pdf
Netball KNEE Australia https://knee.netball.com.au/resources
-
Option two: Call us on
 8356 1000 and organise a time for a call back from one of our physios for a discussion with you about your problem.
8356 1000 and organise a time for a call back from one of our physios for a discussion with you about your problem.